|
|
|
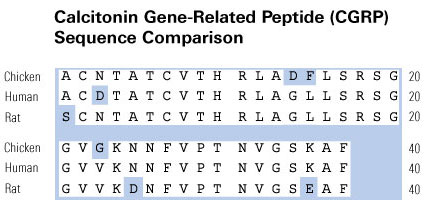
Calcitonin Gene Related Peptide (CGRP) |
New Tumor Biomarker, Cardiovascular and Alzheimer-related Peptides |
In cystic fibrosis (CF), a lack of functional CF transmembrane conductance regulator (CFTR) chloride channels causes defective secretion by submucosal glands (SMGs), leading to persistent bacterial infection that damages airways and necessitates tissue repair. SMGs are also important niches for slow-cycling progenitor cells (SCPCs) in the proximal airways, which may be involved in disease-related airway repair. Here, we report that calcitonin gene-related peptide (CGRP) activates CFTR-dependent SMG secretions and that this signaling pathway is hyperactivated in CF human, pig, ferret, and mouse SMGs. Since CGRP-expressing neuroendocrine cells reside in bronchiolar SCPC niches, we hypothesized that the glandular SCPC niche may be dysfunctional in CF. Consistent with this hypothesis, CFTR-deficient mice failed to maintain glandular SCPCs following airway injury. In wild-type mice, CGRP levels increased following airway injury and functioned as an injury-induced mitogen that stimulated SMG progenitor cell proliferation in vivo and altered the proliferative potential of airway progenitors in vitro. Components of the receptor for CGRP (RAMP1 and CLR) were expressed in a very small subset of SCPCs, suggesting that CGRP indirectly stimulates SCPC proliferation in a non-cell-autonomous manner. These findings demonstrate that CGRP-dependent pathways for CFTR activation are abnormally upregulated in CF SMGs and that this sustained mitogenic signal alters properties of the SMG progenitor cell niche in CF airways. This discovery may have important implications for injury/repair mechanisms in the CF airway.
Xie W, Fisher JT, Lynch TJ et al. J Clin Invest. 2011 Aug;121(8):3144-58. doi: 10.1172/JCI41857. Epub 2011 Jul 18.
Purpose: The aim of our study was to assess the variation of CGRP* expression in patients with IDC and in patients with IDC+DCIS in relation with % mammographic breast density (BD), the uptake of the cell proliferation seeking radiotracer 99mTc-(V)DMSA (SMM uptake), the proliferation index (Ki -67) and the estrogen receptors (ER) status.
Methods: We studied retrospectively 24 women who referred to our department with suspicious findings on palpation and/or mammography and were evaluated preoperatively with 99mTc-(V)DMSA scintimammography. Histology revealed 12 IDC (mean age ± SD = 66.5 ± 13.1) and 12 IDC + DCIS (mean age ± SD = 58.5 ± 15.1). Immunohistochemical staining for CGRP*, Ki-67 and ER status was performed in all 24 surgical specimens. BD and SMM uptake were calculated by computer assisted methods and were correlated with CGRP* expression by linear regression analysis. CGRP* values were compared (Mann Whitney test) between patients with >25% and <25% BD. BD and SMM uptake were compared between CGPR*(-) and CGRP*(+) patients and between IDC and IDC + DCIS. Ki-67 and ER were compared between IDC and IDC + DCIS. Ki-67 was also compared between patients with BD >25% and <25%, whereas ER was correlated with CGRP*.
Results: Overall positive correlation was found between BD and CGRP* expression (r = 0.577 p<0.001) [rBD(IDC)-CGRP* = 0.765 p<0.001, rBD(IDC+DCIS)-CGRP* = 0.746 p<0.001]. Positive correlation was found between SMM uptake and CGRP* only in IDC + DCIS [rSMM(IDC+DCIS)-CGRP*= 0.634 p<0.05]. CGRP* expression was significantly higher in patients with >25% BD compared to the ones with <25% (23.18 ± 7.5 vs. 9 ± 5.1 ,p=0.00008). BD and SMM uptake was significantly higher in CGRP*(+) than in CGRP*(-) patients (30.68 ± 11.24 vs. 18.01 ± 4.5 ,p=0.001 and 22.63 ± 10.61 vs. 11.92 ± 4.79, p= 0,012, respectively) as well as in IDC + DCIS as compared to pure IDC (31.38 ± 8.19 vs. 21.67 ± 11.6, p= 0.044 and 27.94 ± 8.04 vs. 13.19 ± 6.84, p=0.0002, respectively). Ki -67 was significantly higher in IDC + DCIS than in pure IDC (27.91 ± 13.8 vs. 12.8 ± 9.44) as well as in patients with BD>25% than in patients with BD<25% (26 ± 15.44 vs. 10 ± 1.63). On the contrary, ER was significantly lower in IDC + DCIS compared to pure IDC (71.81 ± 95.45 vs. 162.17 ± 55.49) and strongly inversely correlated with CGRP* in pure IDC (r=-0.742,p<0.01).
Conclusion: ΒD, SMM, CGRP* and Ki-67 expression were significantly increased and ER status significantly decreased in DCIS+IDC as compared to IDC, indicating that the two groups are different entities, the DCIS+IC being more aggressive and ER independent and possibly associated with a pathway linked to stromal involvement and CGRP* activity.
*Phoenix Pharmaceuticals Inc CA - USA. Poster presented by Papantoniou et al.
BACKGROUND: We evaluated the variation of calcitonin gene related peptide (CGRP) expression in patients with mixed invasive with extensive in situ ductal carcinomas (IDC + DCIS) and pure IDC, in relation to mammographic breast density (%BD), proliferation-seeking radiotracer (99m)Tc(V) dimercaptosuccinic acid (DMSA) uptake (scintimammographic-SMM), proliferation index Ki-67, and estrogen receptor (ER) status. We also assessed CGRP expression with histological grade. METHODS: We studied retrospectively 24 women with suspicious findings on mammography who were evaluated preoperatively with (99m)Tc(V)DMSA scintimammography. Histology revealed 12 IDC (grade II in 8, grade III in 4 patients; mean size +/- SD, 2.6 +/- 1.3 cm; mean age +/- SD, 66.5 +/- 13.1 years) and 12 IDC + DCIS (grade II in 6, grade III in 6 patients; DCIS component mean size +/- SD, 5.3 +/- 1.8 cm; IDC component mean size +/- SD, 2.5 +/- 1.1 cm; mean age +/- SD, 58.5 +/- 15.1 years). Immunohistochemistry for CGRP, Ki-67, and ER status was performed in all 24 surgical specimens. BD and SMM were calculated by computer-assisted methods and were statistically correlated with CGRP expression. BD, SMM, Ki-67, and ER were statistically compared between IDC and IDC + DCIS, whereas CGRP, Ki-67, and ER were compared between patients with BD >25 and <25%. CGRP was also compared (t test) between grade II and grade III in both groups. RESULTS: Overall positive correlation was found between BD and CGRP (r = 0.577, P < 0.001). Positive correlation was established between SMM and CGRP only in IDC + DCIS (r (SMM(IDC+DCIS)-CGRP) = 0.634, P < 0.05). CGRP and Ki-67 were significantly higher in patients with BD >25% compared with <25% BD patients (P = 0.00008 and P = 0.014, respectively). BD and SMM were significantly higher in CGRP(+) than in CGRP(-) patients as well as in IDC + DCIS compared with IDC. Ki-67 was significantly higher, whereas ER was significantly lower, in IDC + DCIS than in IDC. In all patients, CGRP was significantly higher in grade II as compared with grade III (P = 0.005). In the mixed group (IDC + DCIS), grade II cancers had also significantly higher CGRP values as compared with grade III ones (P = 0.004). In pure IDC, no statistical difference was found between grade II and III (P = 0.4). CONCLUSIONS: BetaD, SMM, CGRP, and Ki-67 were significantly increased, whereas ER was significantly decreased, in IDC + DCIS as compared with IDC, indicating that IDC + DCIS is an entity that is more aggressive, ER independent, and possibly associated with a pathway linked to stromal involvement and CGRP activity.
Papantoniou et al. Breast Cancer. 2010 Feb 9. [Epub ahead of print]
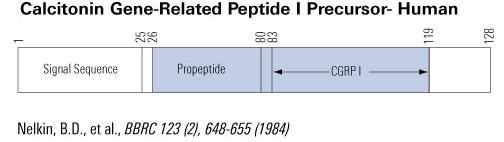
The calcitonin/CGRP multigene complex encodes a family of peptides: calcitonin, its C-terminal flanking peptide, katacalcin, and a third novel peptide, calcitonin gene-related peptide (CGRP). The 32-amino acid peptide calcitonin inhibits the osteoclast, thereby conserving skeletal mass during periods of potential calcium lack, such as pregnancy, growth, and lactation. This hormonal role is emphasized by observations that lower circulating calcitonin levels are associated with bone loss and that calcitonin replacement prevents further bone loss. Structurally, CGRP resembles calcitonin and has been implicated in neuromodulation and in the physiological regulation of blood flow. Here we review the molecular genetics, structure, and function of the calcitonin-gene peptides as analyzed in the laboratory and focus on more recent clinical studies relating to disorders and therapeutics.
Zaidi et al. Crit Rev Clin Lab Sci. 1990;28(2):109-74.
|
|
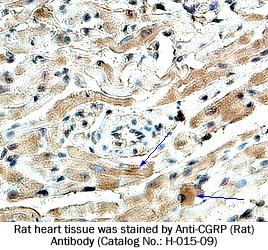
Fixative |
10% formalin |
Embedding |
Paraffin |
Negative Control |
No primary antibody |
Pretreatment |
N/A |
Blocking |
2% Normal Goat Serum |
Primary Antibody |
Rabbit Anti-CGRP (Rat) Antiserum (Catalog No.:H-015-09) |
Optimal Dilution |
1:200 (1hour at RT) |
Secondary Antibody |
Goat Anti-Rabbit IgG, Biotinylated (1:400), 30 min |
Amplification |
ABC (Vector) (1:400, 30 min) |
Detection System |
HRP |
Substrate |
DAB (Sigma), 3 min |
Counterstained |
Hematoxylin, 30 sec |
Papantoniou et al used the CGRP (Human) RIA Kit to show a possible link between CGRP and breast cancer.
 | 
|
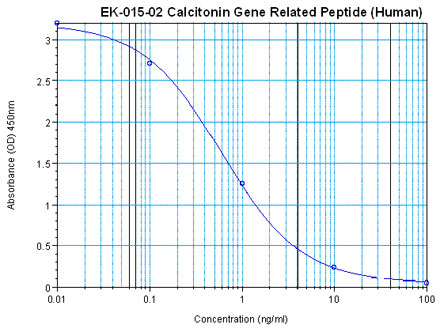
Linear Range: 0.28-3.38 ng/ml |
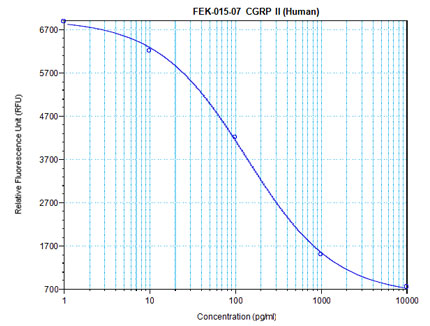
Linear Range: 60-1186 pg/ml
4.6 times more sensitive than normal EIA Kit |
| 
|
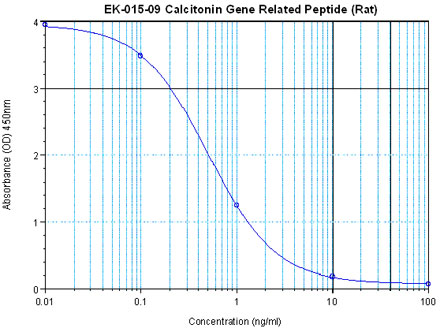
Linear Range: 0.19-2.32 ng/ml |
Linear Range: 29.2-668 pg/ml
5 times more sensitive than normal EIA Kit |
| 
|
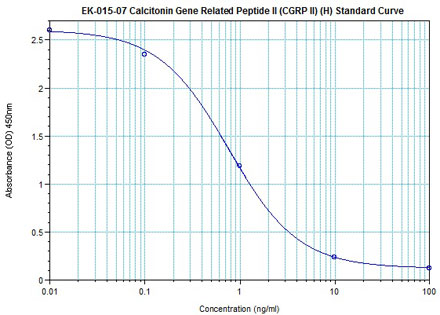
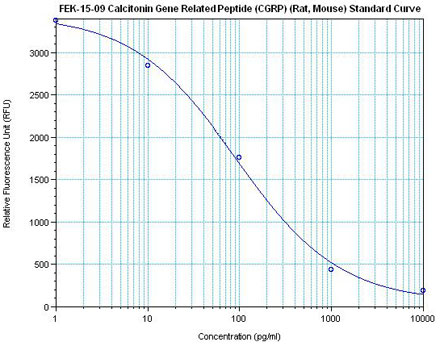
Linear Range: 0.16-1.81 ng/ml |
Linear Range: 46-452 pg/ml
3 times more sensitive than normal EIA Kit |
|
|
|
%cgrp%
|
|
|